Dr. Hodge, our Medical Director, is available every Wednesday from 12-4 PM at our Sarasota, FL office. FOR A LIMITED TIME the initial visit is being offered at an introductory special price of $169, normally this service is $199! For those who already have a card, Re-Certification is available at a price of $99. You can book your visit today using our online booking form below or call our office to schedule your visit at: (941) 806-5511
HISTORY OF CANNABIS AS A MEDICINE
History of Cannabis as a Medicine
By Lester Grinspoon, M.D.,
August 16, 2005
A native of Central Asia, cannabis may have been cultivated as much as 10,000 years ago. It was certainly cultivated in China by 4000 B.C. and in Turkestan by 3000 B.C. It has long been used as a medicine in India, China, the Middle East, Southeast Asia, South Africa, and South America. The first evidence of the medicinal use of cannabis is in an herbal published during the reign of the Chinese Emperor Chen Nung 5000 years ago. It was recommended for malaria, constipation, rheumatic pains, 'absentmindedness' and 'female disorders.'. Another Chinese herbalist recommended a mixture of hemp, resin, and wine as an analgesic during surgery. In India cannabis has been recommended to quicken the mind, lower fevers, induce sleep, cure dysentery, stimulate appetite, improve digestion, relieve headaches, and cure venereal disease. In Africa, it was used for dysentery, malaria, and other fevers. Today certain tribes treat snakebite with hemp or smoke it before childbirth. Hemp was also noted as a remedy by Galen and other physicians of the classical and Hellenistic eras, and it was highly valued in medieval Europe. The English clergyman Robert Burton, in his famous work The Anatomy of Melancholy, published in 1621, suggested the use of cannabis in the treatment of depression. The New English Dispensatory of 1764 recommended applying hemp roots to the skin for inflammation, a remedy that was already popular in eastern Europe. The Edinburgh New Dispensary of 1794 included a long description of the effects of hemp and stated that the oil was useful in the treatment of coughs, venereal disease, and urinary incontinence. A few years later the physician Nicholas Culpeper summarized all the conditions for which cannabis was supposed to be medically useful.
But in the West cannabis did not come into its own as a medicine until the mid-nineteenth century. During its heyday, from 1840 to 1900, more than 100 papers were published in the Western medical literature recommending it for various illnesses and discomforts. It could almost be said that physicians of a century ago knew more about cannabis than contemporary physicians do; certainly, they were more interested in exploring its therapeutic potential.
The first Western physician to take an interest in cannabis as a medicine was WB O'Shaughnessy, a young professor at the Medical College of Calcutta, who had observed its use in India. He gave cannabis to animals, satisfied himself that it was safe, and began to use it with patients suffering from rabies, rheumatism, epilepsy, and tetanus. In a report published in 1839, he wrote that he had found tincture of hemp (a solution of cannabis in alcohol, taken orally) to be an effective analgesic. He was also impressed with its muscle-relaxant properties and called it 'an anticonvulsant remedy of the greatest value.'
O'Shaughnessy returned to England in 1842 and provided cannabis to pharmacists. Doctors in Europe and the United States soon began to prescribe it for a variety of physical conditions. Cannabis was even given to Queen Victoria by her court physician. It was listed in the United States Dispensatory in 1854 (with a warning that large doses were dangerous and that it was a powerful 'narcotic') Commercial cannabis preparations could be bought in drugstores. During the Centennial Exposition of 1876 in Philadelphia, some pharmacists carried ten pounds or more of hashish.
Meanwhile, reports on cannabis accumulated in the medical literature. In 1860, Dr. RR M'Meens reported the findings of the Committee on Cannabis Indica to the Ohio State Medical Society. After acknowledging a debt to O'Shaughnessy, M'Meens reviewed symptoms and conditions for which Indian hemp had been found useful, including tetanus, neuralgia, dysmenorrhea (painful menstruation), convulsions, the pain of rheumatism and childbirth, asthma, postpartum psychosis, gonorrhea, and chronic bronchitis. As a hypnotic (sleep-inducing drug) he compared it to opium: "Its effects are less intense, and the secretions are not so much suppressed by it. Digestion is not disturbed; the appetite rather increased; ... The whole effect of hemp being less violent, and producing a more natural sleep, without interfering with the actions of the internal organs, it is certainly often preferable to opium, although it is not equal to that drug in strength and reliability." Like O'Shaughnessy, M'Meens emphasized the remarkable capacity of cannabis to stimulate appetite.
Interest persisted into the next generation. In 1887, HA Hare extolled the capacity of hemp to subdue restlessness and anxiety and distract a patient's mind in terminal illness. In these circumstances, he wrote, "The patient, whose most painful symptom has been mental trepidation, may become more happy or even hilarious." He believed cannabis to be as effective a pain reliever as opium: "During the time that this remarkable drug is relieving pain, a very curious psychical condition sometimes manifests itself; namely, that the diminution of the pain seems to be due to its fading away in the distance, so that the pain becomes less and less, just as the pain in a delicate ear would grow less and less as a beaten drum was carried farther and farther out of the range of hearing. Hare also noted that hemp is an excellent topical anesthetic, especially for the mucous membranes of the mouth and tongue -- a property well known to dentists in the nineteenth century.
In 1890, JR Reynolds, a British physician, summarized 30 years of experience with Cannabis indica, recommending it for patients with "senile insomnia" "In this class of cases I have found nothing comparable in utility to a moderate dose of Indian hemp." According to Reynolds, hemp remained effective for months and even years without an increase in the dose. He also found it valuable in the treatment of various forms of neuralgia, including tic douloureux (a painful facial neurological disorder), and added that it was useful in preventing migraine attacks: "Very many victims of this malady have for years kept their suffering in abeyance by taking hemp at the moment of threatening or onset of the attack." He also found it useful for certain kinds of epilepsy, for depression, and sometimes for asthma and dysmenorrhea.
Dr. JB Mattison in 1891 called it... "a drug that has a special value in some morbid conditions and the intrinsic merit and safety of which entitles it to a place it once held in therapeutics." Mattison reviewed its uses as an analgesic and hypnotic, with special reference to dysmenorrhea, chronic rheumatism, asthma, gastric ulcer, and morphine addiction, but for him the most important use of cannabis was treating "that opprobrium of the healing art -- migraine." Revealing his own and earlier physicians' experiences, he concluded that cannabis not only blocks the pain of migraine but prevents migraine attacks. Years later William Osler expressed his agreement, saying that cannabis was "probably the most satisfactory remedy" for migraine.
Mattison's report concluded on a wistful note:
Dr. Suckling wrote me: "The young men are rarely prescribing it.". To them I specially commend it. With the wish for speedy effect, it is so easy to use that modern mischief maker, hypodermic morphia, that they [young physicians] are prone to forget remote results of incautious opiate giving. Would that the wisdom which has come to their professional fathers through, it may be, a hapless experience might serve them to steer clear of narcotics shoals on which many a patient has gone awreck. Indian hemp is not here lauded as a specific. It will, at times fail. So do other drugs. But the many cases in which it acts well entitle it to a large and lasting confidence.
As he noted, the medical use of cannabis was already in decline by 1890. The potency of cannabis preparations was too variable, and individual responses to orally ingested cannabis seemed erratic and unpredictable. Another reason for the neglect of research on the analgesic properties of cannabis was the greatly increased use of opiates after the invention of the hypodermic syringe in the 1850s, which allowed soluble drugs to be injected for fast relief of pain; hemp products are insoluble in water and so cannot easily be administered by injection. Toward the end of the 19th century, the development of such synthetic drugs as aspirin, chloral hydrate, and barbiturates, which are chemically more stable than Cannabis indica and therefore more reliable, hastened the decline of cannabis as a medicine. But the new drugs had striking disadvantages. More than a thousand people die from aspirin-induced bleeding each year in the United States, and barbiturates are, of course, far more dangerous. One might have expected physicians looking for better analgesics and hypnotics to turn to cannabinoid substances, especially after 1940, when it became possible to study congeners (chemical relatives) of tetrahydrocannabinol that might have more stable and specific effects.
But the Marihuana Tax Act of 1937 undermined any such experimentation. This law was the culmination of a campaign organized by the Federal Bureau of Narcotics under Harry Anslinger in which the public was led to believe that marihuana was addictive and that its use led to violent crimes, psychosis, and mental deterioration. The film Reefer Madness, made as part of Anslinger's campaign, may be a joke to the sophisticated today, but it was once regarded as a serious attempt to address a social problem, and the atmosphere and attitudes it exemplified and promoted continue to influence our culture today.
Under the Marihuana Tax Act, anyone using the hemp plant for certain defined industrial or medical purposes was required to register and pay a tax of a dollar an ounce. A person using medical marijuana for any other purpose had to pay a tax of $100 an ounce on unregistered transactions. Those who failed to comply were subject to large fines or prison for tax evasion. The law was not directly aimed at the medical use of marijuana -- its purpose was to discourage recreational marijuana smoking. It was put in the form of a revenue measure to evade the effect of Supreme Court decisions that reserved to the states the right to regulate most commercial transactions. By forcing some marijuana transactions to be registered and others to be taxed heavily, the government could make it prohibitively expensive to obtain the drug legally for any other than medical purposes. Almost incidentally, the law made medical use of cannabis difficult because of the extensive paperwork required of doctors who wanted to use it. The Federal Bureau of Narcotics followed up with "anti-diversion" regulations that contributed to physicians' disenchantment. Cannabis was removed from the United States Pharmacopeia and National Formulary in 1941.
In the 1960s, as large numbers of people began to use marijuana recreationally, anecdotes about its medical utility began to appear, generally not in the medical literature but in the form of letters to popular magazines like Playboy. Meanwhile, legislative concern about recreational use increased, and in 1970 Congress passed the Comprehensive Drug Abuse Prevention and Control Act (also called the Controlled Substances Act), which assigned psychoactive drugs to five schedules and placed cannabis in Schedule 1, the most restrictive. According to the legal definition, Schedule I drugs have no medical use and a high potential for abuse, and they cannot be used safely even under a doctor's supervision. By that time the renaissance of interest in cannabis as a medicine was well underway. Two years later, in 1972, the National Organization for the Reform of Marijuana Laws (NORML) petitioned the Bureau of Narcotics and Dangerous Drugs (formerly the Federal Bureau of Narcotics) to transfer marijuana to Schedule II so that it could be legally prescribed by physicians.
The hearings before the Bureau of Narcotics and Dangerous Drugs (BNDD) were instructive. As I waited to testify on the medical uses of cannabis, I witnessed the effort to place pentazocine (Talwin), a synthetic opioid analgesic made by Winthrop Pharmaceuticals, on the schedule of dangerous drugs. The testimony indicated several hundred cases of addiction, a number of overdose deaths, and considerable evidence of abuse. Six lawyers from the drug company, briefcases in hand, came forward to prevent the classification of pentazocine, or at least ensure that it was placed in one of the less restrictive schedules. They succeeded in part; it became a Schedule IV drug, available by prescription with minor restrictions. In the testimony on cannabis, the next drug to be considered, there was no evidence of overdose deaths or addiction -- simply many witnesses, both patients and physicians, testifying to its medical utility. The government refused to transfer it to Schedule II. Might the outcome have been different if a large drug company with enormous financial resources had a commercial interest in cannabis?
In rejecting the NORML petition, the Bureau of Narcotics and Dangerous Drugs failed to call for public hearings, as required by the law. The reason it gave was that reclassification would violate US treaty obligations under the United Nations Single Convention on Narcotic Substances. NORML responded in January 1974 by filing a suit against the BNDD. The US Second Circuit Court of Appeals reversed the bureau's dismissal of the petition, remanding the case for reconsideration and criticizing both the bureau and the Department Of Justice. In September 1975, the Drug Enforcement Administration (DEA), successor to the BNDD, acknowledged that treaty obligations did not prevent the rescheduling of marijuana but continued to refuse public hearings. NORML again filed suit. In October 1980, after much further legal maneuvering, the Court of Appeals remanded the NORML petition to the DEA for reconsideration for the third time.
The government reclassified synthetic tetrahydrocannabinol (dronabinol) as a Schedule II drug in 1985 but kept marijuana itself - - and the tetrahydrocannabinol derived from marijuana (a chemical identical to the synthetic version) - - in Schedule I. Finally, in May 1986 the DEA Administrator announced the public hearings ordered by the court seven years earlier. Those hearings began in the summer of 1986 and lasted two years.
The lengthy hearings involved many witnesses, including both patients and physicians, and thousands of pages of documentation. The record of these hearings constitutes one of the most extensive recent explorations of the evidence on cannabis as a medicine. Administrative law judge Francis L. Young reviewed the evidence and rendered his decision on September 6, 1988. Young said that approval by a "significant minority" of physicians was enough to meet the standard of "currently accepted medical use in treatment in the United States" established by the Controlled Substances Act for a Schedule II drug. He added that 'marijuana, in its natural form, is one of the safest therapeutically active substances known to man.. One must reasonably conclude that there is accepted safety for use of marijuana under medical supervision. To conclude otherwise, on the record, would be unreasonable, arbitrary, and capricious.' Young went on to recommend “that the Administrator [of the DEA] conclude that the marijuana plant considered as a whole has a currently accepted medical use in treatment in the United States, that there is no lack of accepted safety for use of it under medical supervision and that it may lawfully be transferred from Schedule I to Schedule II."
In determining what "currently accepted medical use" meant for legal purposes, Judge Young was adopting the view of petitioners and rejecting that of the DEA, whose criteria were the result of a previous legal challenge involving the drug 3,4-methylenedioxymethamphetamine(MDMA). In 1984 the DEA placed this previously unscheduled drug in Schedule I. The placement was challenged by me and some fellow physicians who believed that MDMA had therapeutic potential. After exhaustive hearings, the administrative law judge rejected the DEA's position that MDMA had no accepted medical use in treatment in the United States and agreed with the challengers that it should be placed in Schedule III rather than Schedule I. The DEA administrator rejected this recommendation. We appealed to the US First Circuit Court of Appeals, which ruled in our favor, finding that formal approval for marketing by the Food and Drug Administration, the DEA's criterion for "accepted medical use in treatment in the United States," was unacceptable under the terms of the Controlled Substances Act.
The DEA administrator responded with the following new criteria for accepted medical use of a drug: (1) scientifically determined and accepted knowledge of its chemistry; (2) scientific knowledge of its toxicology and pharmacology in animals; (3) effectiveness in human beings established through scientifically designed clinical trials; (4) general availability of this substance and information about its use; (5) recognition of its clinical use in generally accepted pharmacopeia, medical references, journals, or textbooks; (6) specific indications for the treatment of recognized disorders; (7) recognition of its use by organizations or associations of physicians; and (8) recognition and use by a substantial segment of medical practitioners in the United States. These were the criteria rejected by Judge Young in his marijuana decision.
The DEA disregarded the opinion of the administrative law judge and refused to reschedule marijuana. The agency's lawyer remarked, "The judge seems to hang his hat on what he calls a respectable minority of physicians. What percent are you talking about? One half of one per cent? One quarter of one percent?". DEA Administrator John Lawn went further, calling claims for the medical utility of marijuana a "dangerous and cruel hoax." In March 1991 the plaintiffs appealed yet again and in April the District of Columbia Court of Appeals unanimously ordered the DEA to re-examine the standards, suggesting that they were illogical and that marijuana could never satisfy them. An illegal drug could not be used by a substantial number of doctors or cited as a remedy in medical texts. As the court pointed out, "We are hard-pressed to understand how one could show that any Schedule I drug was in general use or generally available.". The court returned the case to the DEA for further explanation, but it offered no direct challenge to the central dogma that marijuana lacks therapeutic value. The DEA issued a final rejection of all pleas for reclassification in March 1992.
Despite the obstructionism of the federal government, a few patients have been able to obtain marijuana legally for therapeutic purposes. State governments began to respond in a limited way to pressure from patients and physicians in the late 1970s. In 1978, New Mexico enacted the first law designed to make marijuana available for medical use. Thirty-three states followed in the late 1970s and early 1980s. In 1992, Massachusetts became the 34th state to enact such legislation, and in 1994 Missouri became the 35th.
But the laws proved difficult to implement. Because marijuana is not recognized as a medicine under federal law, states can dispense it only by establishing formal research programs for getting FDA approval for an Investigational New Drug (IND) application. Many states gave up as soon as the officials in charge of the programs confronted the regulatory nightmare of the relevant federal laws. Nevertheless, between 1978 and 1984, 17 states received permission to establish programs for the use of marijuana in treating glaucoma and the nausea induced by cancer chemotherapy. Each of these programs fell into abeyance because of the many problems involved.
Take the case of Louisiana, where a law was passed in 1978 establishing a program that allowed a Marijuana Prescription Board to review and approve applications by physicians to treat patients with cannabis. The board would have preferred a simple procedure in which medical decisions would be entrusted to the practicing physician, but federal agencies would not supply cannabis without an IND. That would have required an enormous amount of paperwork and would have made the program intolerably cumbersome. The board therefore decided to use an already approved research program operated by the National Cancer
Institute, which was limited to cancer patients and employed only a synthetic THC. Marijuana itself was not made legally available to any patient in Louisiana. With these limitations, the program proved ineffective. Patients felt compelled to use illicit cannabis, and at least one was arrested.
Only ten states eventually established programs in which cannabis was used as a medicine. Among these New Mexico was the first and most successful, largely because of the efforts of the young cancer patient, Lynn Pierson. In 1978 the state legislature enacted a law allowing physicians to prescribe marijuana to patients suffering from nausea and vomiting induced by cancer chemotherapy. The law was later modified to comply with federal IND regulations requiring a research program. Considerable friction immediately developed between the FDA and the people in charge of the New Mexico program. The FDA demanded studies with placebos (inactive substances) as control; the physicians in the New Mexico program wanted to provide sick patients with care. The FDA wanted to proceed slowly, the attitudes of the physicians reflected the urgency of their patients' needs. Eventually a compromise was reached: patients would be assigned at random to treatment with marijuana cigarettes or synthetic THC capsules. But the prolonged delay suggested to the New Mexico officials that the FDA was not dealing in good faith, and tensions began to grow. At one point state officials even considered using confiscated marijuana, and the chief of the State Highway Patrol was asked whether it could be supplied.
In August 1978, Lynn Pierson, who had made a heroic effort to establish a compassionate program, died of cancer without ever having received legal marijuana. Now the FDA approved the New Mexico IND, only to rescind the approval a few weeks later, after the public furor surrounding Pierson's death had faded. At that point New Mexico officials considered holding a press conference to condemn federal officials for "unethical and immoral behavior.". Finally, in November 1978, the program was approved, supplies of marijuana were promised within a month, but not delivered for two months.
The random design of the program was soon violated. Patients discussed among themselves the relative merits of the two types of treatment and switched when they wanted to do so; this also gave them a sense of control over their own care. But many patients believe, despite the denials of the National Institute of Drug Abuse (NIDA), that the cigarettes they received were not of adequate potency. The state never conducted an independent assay. Some patients left the program in order to buy cannabis on the streets, which they felt was better than either government marijuana or synthetic THC.
From 1978 to 1986 about 250 cancer patients in New Mexico received either marijuana or THC after conventional medications had failed to control their nausea and vomiting. For these patients both marijuana and THC were effective, but marijuana was superior. More than 90% reported significant or total relief from nausea and vomiting. Only three adverse effects were reported in the entire program -- anxiety reactions that were easily treated by simple reassurance.
The successful programs in other states resembled the one in New Mexico. It was understood that "research" was merely a disguise; the aim was to relieve suffering. Although the results did not meet the methodological standards for controlled clinical research, they did confirm the effectiveness of cannabis and the advantage of smoked marijuana over oral THC. Incidentally, none of the programs reported problems with abuse or the diversion of either THC or marijuana cigarettes.
A New York State Department of Health report on the therapeutic use of cannabis asked why more patients and physicians had not enrolled in the New York program. It concluded that there were several reasons. First, physicians were skeptical because of their limited training and experience. Second, bureaucratic obstacles were enormous. As the report states, "Hospital pharmacists and administrators complain about paperwork and procedures. Physicians complain about burdensome reporting and application requirements.
At least 16 physicians have inquired into the availability of marijuana, but have chosen not to enroll in the program because they perceive a large amount of bureaucratic procedure." A third possibility was that many patients and physicians decided it was easier to get marijuana of good quality on the street.
At about the same time the state programs were being instituted, growing demand forced the FDA to institute an Individual Treatment IND (commonly referred to as a Compassionate Use IND or Compassionate IND) for the use of individual physicians whose patients needed marijuana. The application process was not easy, because it was designed for an entirely different purpose -- making pharmaceutical companies assure the safety of new drugs. First the patient in need of cannabis had to persuade a physician to apply to the FDA for an IND. The physician had to file a special form with the DEA covering Schedule I drugs. If the application was approved by both agencies, the physician then had to fill out special order forms for marijuana, which were sent to the National Institute on Drug Abuse (NIDA). NIDA grows cannabis on a farm at the University of Mississippi -- the only legal marijuana farm in the United States -- and sends it to North Carolina, where it is rolled into cigarettes that were supposed to have the same potency as street marijuana (at that time 2%, presently 3.5%). NIDA then shipped the marijuana to a designated pharmacy that had to comply with stringent DEA regulations for drug security. The application process took four to eight months. Both the FDA and the DEA required constant prodding and rarely responded within the time specified by law. According to the (now defunct) Alliance for Cannabis Therapeutics, which helped a number of patients and physicians through the process, government agencies routinely seemed to lose some of the application forms, and the doctor had to resubmit them, sometimes more than once. Understandably, most physicians did not want to become entangled in the paperwork, especially since many also believe there is some stigma attached to prescribing marijuana.
In 1976 Robert Randall, who suffered from glaucoma, became the first patient to receive a Compassionate IND for the use of marijuana. Over the next 13 years the government reluctantly awarded a half dozen more. Then, in 1989 the FDA was deluged with applications from people with AIDS. The case that called attention to the absurd and appalling consequences of the medical ban on marijuana was the government assault on Kenneth and Barbra Jenks, a Florida couple in their 20s who contracted AIDS through a blood transfusion given to the husband, a hemophiliac. Both were suffering from nausea, vomiting, and appetite loss caused by AIDS or AZT; their doctor feared that Barbra Jenks would die of starvation before the disease killed her. In early 1989 the Jenkses learned about marijuana through a support group for people with AIDS. They began to smoke it and for a year they led a fairly normal life. They felt better, regained lost weight, and were able to stay out of the hospital; Kenneth Jenks even kept his full-time job.
Then someone informed on them. On March 29, 1990, 10 armed narcotics officers battered down the door of their trailer home, held a gun to Barbra Jenks's head, and seized the evidence of crime, two small marijuana plants they had been growing because they could not afford to pay the street price of the drug. Cultivation of marijuana is a felony in Florida; the Jenkses faced up to five years in prison. At their trial in July they used the defense of medical necessity, which is rarely successful. The judge rejected this defense and convicted the Jenkses, although he imposed only a suspended sentence. The conviction was later overturned by a higher court and the defense of medical necessity was sustained.
The case received national publicity and the Jenkses were able to obtain a Compassionate IND. Now the FDA was inundated with new requests from AIDS sufferers. The number of extant Compassionate IND's rose from five to thirtyfour in a year. Then James O. Mason, chief of the Public Health Service, announced that the program would be suspended because it undercut the Bush administration opposition to the use of the illegal drugs. "If it is perceived that the Public Health Service is going around giving marijuana to folks, there would be to a perception that this stuff can't be so bad," Mason said. He went on, "It gives a bad signal. I don't mind doing that if there is no other way of helping these people... But there is not a shred of evidence that smoking marijuana assists a person with AIDS."
After keeping the program "under review" for nine months, the Public Health Service discontinued it in March 1992. Twenty eight patients whose applications had already been approved were denied the promised marijuana. Thirteen patients already receiving marijuana were allowed to continue receiving it. Presently, the number has fallen to seven. After more than 20 years in which hundreds of people have worked through state legislatures, federal courts, and administrative agencies to make marijuana available for suffering people, these seven are the only ones for whom it is not still a forbidden medicine.
With the demise of the Compassionate IND program, the last flicker of compassion toward medical marijuana patients on the part of the federal government disappeared. Now there was no hope of any kind of legal access to a drug that thousands of Americans had come to believe was the best treatment for their particular medical problems. Again, some of the states began to try to fill the vacuum beginning with California which in 1996 passed Proposition 215. This voter initiative made it possible for patients with specified symptoms and syndromes for which cannabis is useful to obtain from a physician a letter which is the functional equivalent of a prescription for marijuana. These "prescriptions" are "filled" at one of the many nonprofit "Compassion Clubs" which have sprung up in the 10 states which, through legislation or voter initiative, have now made similar allowances for medical marijuana patients. The government has responded with a determined campaign aimed at closing down the Compassion Clubs, and many patients who had finally found a legitimate way to obtain this medicine were again dependent on illicit sources or forced to grow their own, and some were prosecuted.
If herbal marihuana is without any medical utility, as the US government claims, why would thousands of patients risk running afoul of the law to obtain and use it? They use it for one or more of three reasons: (1) herbal marihuana is, even with the prohibition tariff, less expensive than either the conventional medicine it replaces or Marinol; (2) because its toxicity is so low, they suffer fewer "side effects" (toxic effects) than they do with the conventional medicine for which cannabis has been substituted; and (3) because it is remarkably versatile it is useful in the treatment of a number of syndromes and symptoms. Today, herbal marihuana is most commonly, but certainly not exclusively, used in the treatment of:
The Severe Nausea and Vomiting of Cancer Chemotherapy
Glaucoma
Epilepsy
Multiple Sclerosis
The Spasm and Pain of Paraplegia and Quadriplegia
AIDS
Chronic Pain
Migraine
Rheumatic Diseases (Osteoarthritis and Ankylosing Spondylitis)
Premenstrual Syndrome, Menstrual Cramps, and Labor Pains
Ulcerative Colitis
Crohn's Disease
Phantom Limb Pain
Depression
Hyperemesis Gravidarum
There are several reasons why medicine has not been quicker to recognize the value of readmitting cannabis to the pharmacopeia. One is the lack of incentive of pharmaceutical companies to develop it as a medicine because it is not possible to patent a plant. In fact, there is a disincentive because this versatile medicine would successfully compete with many of their extant products. But the most important reason is the low regard with which medicine holds anecdotal data, and almost all that we know about herbal marijuana as a medicine is anecdotal. Anecdotal data is less reliable than that derived from double-blind controlled studies which were introduced in the early 60s and which modern medicine now relies on. Still, it must not be forgotten that modern medicine was built upon a foundation of anecdotal data and it continues to point to new therapeutic possibilities, some of which, as in the case of cannabis, turn out to be valuable. Now, attitudes toward the anecdotal nature of most of the data on cannabis are slowly changing. In a paper recently published in Trends in Neurosciences (May, 2005) the authors write as follows:
Use of cannabis as a medicine for numerous conditions has a well documented history stretching back thousands of years. With the identification of an endogenous system of receptors and ligands in recent years, abundant experimental data have reinforced the anecdotal claims of people who perceive medicinal benefit from the currently illegal consumption of cannabis. This, combined with data from recent clinical trials, points to the prospect of cannabis as a medication in the treatment of multiple sclerosis and numerous other medical conditions.
In the 19th century cannabis was dispensed as an orally administered medicine in the form of an alcohol-based extract generically known as Cannabis indica. Dosage was a matter of guesswork in as much as there were no bioassays at that time. Physicians were not much concerned about over-dosage because while an especially large dose might make a patient uncomfortable until the drug effect wore off, it would not in any way harm the patient. What distressed physicians of this era was the time delay between having the patient take, say, two minems of Tilden's Solution (a commonly used proprietary form of Cannabis indica) and the onset of symptom relief -- about an hour and a half.
Nineteenth-century physicians were unaware of one of the remarkable properties of herbal marijuana e.g. that it could be smoked and when delivered in this way it would provide symptom relief within minutes. This was a discovery made by early twentieth-century recreational users who passed it on to patients who used marijuana as a medicine. It is a critically important medicinal property of cannabis because it allows patients to quickly determine just how much of the drug they need to achieve their medical objective. Additionally, it provides the patient, who is in the best position to determine this dose, the ability to be in control of the relief of his pain, nausea, or other symptom.
While there has never been reported a case of lung cancer or emphysema attributable to the smoking of cannabis, there is in today's widespread antismoking climate concern about the effect of the smoke on the pulmonary system. Another fortuitous property of marijuana is that there is a temperature window which is below the ignition point of cannabis, but within which the cannabinoids will vaporize. There is now generally available a device known as a vaporizer which takes advantage of this property. It holds herbal marihuana at a temperature of between 284 F and 392 F, thus allowing the patient to inhale the therapeutic cannabinoids free of any of the products of the burning plant material, including putative carcinogens.
The medical marijuana problem is a Janus-like conundrum; one view of the problem is seen through the eyes of patients and another through those of their government. One face regards with dismay the problem of denying herbal marihuana to the growing number of pained, impatient patients who find it useful, often more useful, less toxic and cheaper than the legally available medications. Through the patients' eyes the problem is, of course, how to acquire and use this medicine without swelling the ranks (already more than 750,000 annually) of those who are arrested for using this illegal substance and how to avoid jeopardizing job security through random urine testing. The other face, the backward looking one, is that of an obdurate government as it defensively and inconsistently insists that "marijuana is not a medicine", and backs up this illinformed, arrogant position with the full force of its vast legal power as it is presently doing in the state of California.
In 1985 the Food And Drug Administration (FDA) approved dronabinol (Marinol) for the treatment of the nausea and vomiting of cancer chemotherapy. Dronabinol is a solution of synthetic tetrahydrocannabinol in sesame oil (the sesame oil is meant to protect against the possibility that the contents of the capsule could be smoked). Dronabinol was developed by Unimed Pharmaceuticals Inc. with a great deal of financial support from the United States government. This was the first hint that "pharmaceuticalization" of cannabis might be what the government hoped would solve its problems with marijuana as medicine, the problem of how to make the medical properties of cannabis (in so far as the government believes such properties exist) widely available as a medicine while at the same time prohibiting its use for any other purpose. But Marinol did not displace marijuana as "the treatment of choice", most patients found the herb itself much more useful than dronabinol in the treatment of the nausea and vomiting of cancer chemotherapy. In 1992, the treatment of the AIDS wasting syndrome was added to dronabinol"s labeled uses; again, patients reported that it was inferior to smoked herbal marihuana. Because it was thought that it would sell better if placed in a less restrictive Drug Control Schedule, it was moved from Schedule II to Schedule III in the year 2000. But Marinol has not solved the marijuana-as-a-medicine problem because so few of the patients who have discovered the therapeutic usefulness of marijuana use dronabinol. In general, they find it less effective than smoked marijuana, it cannot be titrated because it has to be taken orally which causes a long delay in the manifestation of its therapeutic utility, and even with the prohibition tariff on street marijuana, Marinol is more expensive. Thus, the first attempt at pharmaceuticalization proved not to be the answer. In practice, for many patients who use marijuana as a medicine the doctor-prescribed Marinol serves primarily as a cover from the threat of the growing ubiquity of urine tests.
More recently, the Institute of Medicine (IOM) Report (1999), which acknowledged marijuana's usefulness as a medicine, proposed that the solution was the "pharmaceuticalization" of cannabis: prescription of isolated individual cannabinoids, synthetic cannabinoids and cannabinoid analogs. The IOM Report states that ".. if there is any future for marijuana as a medicine, it lies in its isolated components, the cannabinoids, and their synthetic derivatives." It goes on: "Therefore, the purpose of clinical trials of smoked marijuana would not be to develop marijuana as a licensed drug, but such trials could be a first step toward the development of rapid onset, non-smoked cannabinoid delivery systems."
Some cannabinoids and analogs may indeed have advantages over whole smoked or ingested marijuana in limited circumstances. For example, cannabidiol may be more effective as an anti-anxiety medicine and an anticonvulsant when it is not taken along with tetrahydrocannabinol (THC), which sometimes generates anxiety. Other cannabinoids and analogs may prove more useful than herbal marijuana in some circumstances because they can be administered intravenously. For example, 15 to 20% of patients lose consciousness after suffering a thrombotic or embolic stroke, and some people who suffer brain syndrome after a severe blow to the head become unconscious. The new analog Dexanabinol (HU-211) has been shown to protect brain cells (in anaimals) from damage when given immediately after a stroke; if this proves to be true in humans, it will be possible to give it intravenously to an unconscious person. Presumably other analogs may offer related advantages. Some of these commercial products may also lack the psychoactive effects which make marijuana useful to some for nonmedical purposes. Therefore, they will not be defined as “abusable” drugs subject to the constraints of the Comprehensive Drug Abuse and Control Act. Nasal sprays, vaporizers, nebulizers, skin patches, pills, and suppositories can be used to avoid exposure of the lungs to the particulate matter in marijuana smoke.
The question is whether these developments will make herbal marijuana itself medically obsolete. Surely many of these new products would be useful and safe enough for commercial development. It is uncertain, however, whether pharmaceutical companies will find them worth the enormous development costs. Some may be (for example a cannabinoid inverse agonist that reduces appetite might be highly lucrative), but for most specific symptoms, analogs or combination of analogs are unlikely to be more useful than natural herbal marijuana. Nor are they likely to have a significantly wider spectrum of therapeutic uses, since the natural product contains the compounds (and synergistic combinations of compounds) from which they are derived. For example, the naturally occurring THC and cannabidiol of marijuana, as well as Dexanabinol, protect animal brain cells after a stroke or traumatic injury.
Furthermore, any new analog will have to have an acceptable therapeutic ratio. The therapeutic ratio (an index of the drug's safety) of marijuana is not known because it has never caused an overdose death, but it is estimated, on the basis of extrapolation from animal data, to be an almost unheard of 20,000 to 40,000. The therapeutic ratio of a new analog is unlikely to be higher than that; in fact, new analogs may be much less safe than plant marijuana because it will be physically possible to ingest more of them.
One is compelled to ask, what is the government's problem with medical herbal marijuana? The problem as seen through the eyes of the government is the belief that as growing numbers of people observe relatives and friends using marijuana as a medicine, they will come to understand that this is a drug which does not conform to the description the government has been pushing for years. They will first come to appreciate what a remarkable medicine it really is; it is less toxic than almost any other medicine in the pharmacopeia; it is, like aspirin, remarkably versatile; and it is less expensive than the conventional medicines it displaces. They will then begin to wonder if there are any properties of this drug which justify denying it to people who wish to use it for any reason, let alone arresting more than 750,000 citizens annually. The federal government sees the acceptance of marijuana as a medicine as the gateway to catastrophe, the repeal of its prohibition. In so far as the government views as anathema any use of plant marijuana, it is difficult to imagine it accepting a legal arrangement that would allow its use as a medicine, while at the same time vigorously pursuing a policy of prohibition of any other use. Yet, there are many who believe this type of arrangement is possible and workable. In fact, this is the option the Canadian and Dutch governments are presently pursuing, as are various states in the United States. But it will not be possible to do this in the United States in the absence of large double-blind studies which make use of the medicine that thousands of patients now use, e.g. herbal marijuana.
All of HEALTH, Chronic Health Challenges, and Healing can be boiled down to the 4Ms:
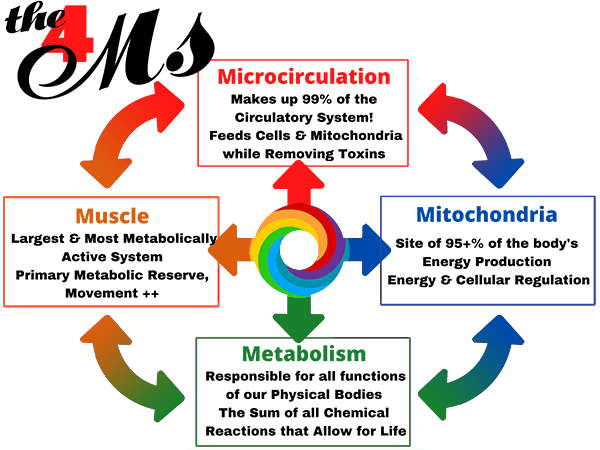
The Microcirculation delivers oxygen & ALL Nutrients to the cells & the Mitochondria.
The Mitochondria make almost ALL the Energy needed to run our Metabolism.
The Metabolism CONTROLS ALL Life Processes.
The Muscles are our primary Metabolic Reserve; Muscles are our primary drivers that build & preserve the Microcirculation & Mitochondria!